
Anterior cruciate ligament injury is the over-stretching or tearing of the anterior cruciate ligament (ACL) in the knee. Athletes who participate in high-demand sports like soccer, football, and basketball are more likely to injure their anterior cruciate ligaments (ACLs).
ACL is one of the major ligaments that help stabilize the knee joint and prevents it from sliding in front of the thigh bone. (A ligament is a tough, flexible band of tissue that holds bones and Cartilage together).
This is a very common knee injury which occurs in sports when there is an over-extension of the knee joint, a quick change in direction while running, when the knee is hit from the side or when one lands incorrectly from a jump. The tear can be partial or complete.
Several studies have shown that female athletes have a higher incidence of ACL injury than male athletes in certain sports. Please note that any injury that can tear the ACL can also possibly injure other ligaments, articular cartilage and the meniscus.
It is common to see ACL injuries combined with damage to the menisci, articular cartilage, collateral ligaments, joint capsule, or a combination of the above. The “unhappy triad,” frequently seen in football players and skiers, consists of injuries to the anterior cruciate ligament (AC), the medial collateral Ligament (MCL), and the medial meniscus.
To enhance the understanding of ACL injury, a little anatomy of the knee joint will help.
Anatomy of the knee joint
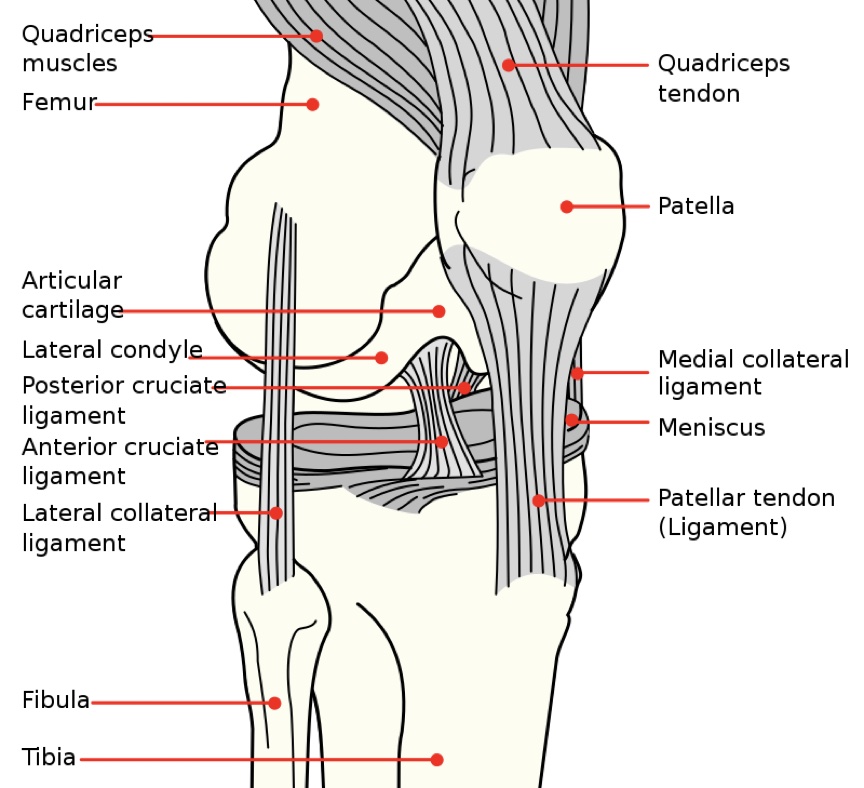
Three bones meet to form the knee joint Viz:
- Thighbone (femur)
- Shinbone (tibia)
- Kneecap (patella)
The kneecap sits in front of the joint to provide some protection.
Bones are connected to other bones by ligaments.
The knee is a hinge joint held together by four ligaments that act like strong ropes to hold the bones together and keep the knee stable.
- Collateral Ligaments
These are found on the sides of the knee and they control the sideways motion of the knee and brace it against unusual movement. The medial collateral ligament (MCL) is on the inside while the lateral collateral ligament (LCL) is on the outside.
- Cruciate Ligaments
These are found inside the knee joint. They cross each other to form an “X” with the anterior cruciate ligament in front and the posterior cruciate ligament in back. The cruciate ligaments control the back-and-forth motion of your knee.
The anterior cruciate ligament runs diagonally in the middle of the knee. It prevents the tibia (the shin bone) from sliding out in front of the femur, as well as provides rotational stability to the knee.
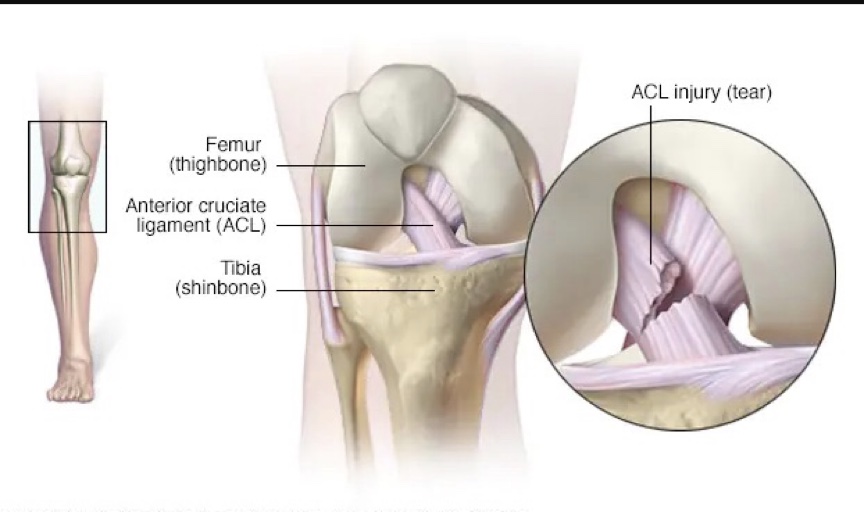
What is Anterior Cruciate Ligament (ACL) Injury?
An anterior cruciate ligament injury is the over-stretching or tearing of the anterior cruciate ligament (ACL) in the knee. A tear may be partial or complete. Although partial tears of the anterior cruciate ligament are rare; most ACL injuries are complete or near complete tears.
 Classification of Anterior Cruciate Ligament (ACL) Injury
Classification of Anterior Cruciate Ligament (ACL) Injury
The ACL injury can be classed into 3 grades viz:
-
Grade 1 Sprain
The ligament is mildly damaged in a Grade 1 Sprain. It has been slightly stretched but is still able to help keep the knee joint stable.
-
Grade 2 Sprain
A Grade 2 Sprain stretches the ligament to the point where it becomes loose. This is often referred to as a partial tear of the ligament.
-
Grade 3 Sprain
This type of sprain is most commonly referred to as a complete tear of the ligament. The ligament has been split into two pieces, and the knee joint is unstable.
Mechanisms of Anterior Cruciate Ligament (ACL) Injury
The mechanism of injury predicts the type of injury. The 2 most common mechanisms are viz:
- In football, when one is tackled from the medial aspect of the knee (inward force), there is external rotation of the knee and flexion thus resulting in medial collateral, anterior cruciate ligament (ACL) and medial meniscal injury.
- When the force is from outside (i.e.) lateral aspect of the knee, the injury is usually to the lateral collateral ligament, anterior cruciate ligament, or both. This is about the most common mechanism.
Risk factors of Anterior Cruciate Ligament (ACL) Injury
There are several factors that increase the risk of an ACL injury viz:
- Being female
Possibly due to differences in anatomy, muscle strength and hormonal influences. The structure of the knee joint in women plays a big role in putting them at a higher risk for an ACL tear— generally, in women, the knee joint has more looseness and range of motion than men’s.
Women also often have less muscle mass around the knee, contributing to more instability, which can lead to a ligament tear if the ligament gets overstretched. Technique differences also play a role.
When coming down from a jump, female athletes tend to land in a collapsing pattern, moving their knees inward and often not bending them enough. This has to do with wider hips which increases the Q –angle ( i.e. the angle between the Hip bone and the patella).
The combination of these factors makes an ACL tear more likely. Also, it has been observed that women have a shallower intercondylar notch which leads to a decreased ACL volume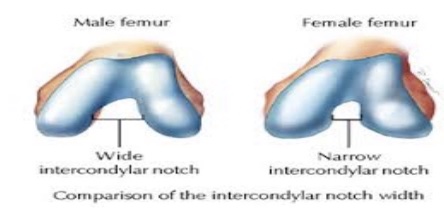
- Participating in certain sports such as soccer, football, basketball, gymnastics and downhill skiing.
- Using faulty movement patterns, such as moving the knees inward during a squat
- Wearing footwear that doesn’t fit properly.
- Using poorly maintained sports equipment, such as ski bindings that aren’t adjusted properly.
- Playing on artificial turf.
Symptoms of Anterior Cruciate Ligament (ACL) Injury
Signs and symptoms of an ACL injury usually include:
- A loud pop or a “popping” sensation in the knee.
- Severe pain and inability to continue an activity.
- Rapid swelling.
- Loss of range of motion.
- A feeling of instability or “giving way” with weight bearing.
How is an Anterior Cruciate Ligament (ACL) Tear Diagnosed?
Diagnosis of an ACL injury starts from:
-
History of the injury
-
Physical exam
During the exam, the health care provider presses on the knee and legs and moves them in certain ways. These tests can show if the ACL is torn.
The Lachman test is the most sensitive physical test for acute anterior cruciate ligament tears. With the patient supine (face up), the examiner supports the patient’s thigh and calf, and the patient’s knee is flexed 20°. The lower leg is moved anteriorly. The excessive passive anterior motion of the lower leg from the femur suggests a significant tear.
-
Imaging tests
- X-ray of the affected Knee
Not every patient requires x-rays. However, anteroposterior, lateral, and oblique x-rays are often taken to exclude fractures.
- MRI
MRI is usually not needed at the initial evaluation. A reasonable approach is to do MRI if symptoms do not resolve after a few weeks of conservative management.
Treatment of Anterior Cruciate Ligament (ACL) Injury
Treatment for an ACL tear varies with the patient’s individual needs. Thus, treatment can be non-surgical or surgical.

-
Nonsurgical Treatment
A torn ACL will not heal without surgery. But nonsurgical treatment may be effective for patients who are elderly or have a very low activity level. If the overall stability of the knee is intact, your doctor may recommend simple, nonsurgical options.
-
RICE Therapy
Do R.I.C.E. therapy immediately after the injury:
-
- R: Rest the affected knee
- I: Ice. (Place some ice block on the injured Knee.
- C: Compression.
- E: Elevation.
-
Bracing
Putting a brace around the knee will keep it stable. Crutches may be given to keep off weight on the injured leg.
-
Physical therapy
As the swelling goes down, a careful rehabilitation program is started. Specific exercises will restore function to the knee and strengthen the leg muscles that support it.
-
Surgical Treatment
The decision to repair an ACL tear with surgery is a function of age, current activity level and desired activity level of the patient. ACL tears cannot be sutured (stitched) back together.
To surgically repair the ACL and restore knee stability, the ligament must be reconstructed. The torn ligament is replaced with a tissue graft. This graft acts as scaffolding for a new ligament to grow on.
Because the regrowth takes time, it may be six months or more before an athlete can return to sports after surgery. Surgery to rebuild an anterior cruciate ligament is done with an arthroscope(a small tube-shaped instrument that is inserted into a joint) using small incisions.
Arthroscopic surgery is less invasive. The benefits of less invasive techniques include less pain from surgery, less time spent in the hospital, and quicker recovery times.
Grafts can be obtained from several sources.
- The patellar tendon runs between the knee cap and the shin bone. This is the “gold standard” for ACL reconstruction. It is often recommended for high-demand athletes and patients whose jobs do not require a significant amount of kneeling.
- Hamstring tendons at the back of the thigh are a common source of grafts.
- Sometimes a quadriceps tendon, which runs from the kneecap into the thigh is used.
- Achilles tendon, semitendinosus, gracilis, or posterior tibialis tendon etc
- Cadaver graft (allograft) can be used.
-
Drug Treatment
Usually, anti-inflammatory medications are prescribed. The natural history of ACL injury if left without surgical intervention varies from patient to patient and depends on the patient’s activity level, degree of injury and instability symptoms.
With a partial ACL tear, recovery is usually within 3 months but a complete ACL tear has unfavourable outcomes without surgical intervention. The reason is obvious, ACL injuries occur in combination with damage to the meniscus, articular cartilage or other ligaments.
Anterior Cruciate Ligament Repair Complications
-
Risk of re-tear
Unfortunately, it’s still possible to re-tear an ACL that was reconstructed and rehabilitated perfectly. The higher the activity level, the higher the risk.
-
Infection
The incidence of infection (HIV, hepatitis B and C) after arthroscopic ACL reconstruction is very low. Post-op deaths have been linked to bacterial infection from allograft (grafts taken from a cadaver) tissue due to improper procurement and sterilization techniques.
-
Growth plate injury
Early ACL reconstruction creates a possible risk of growth plate injury in the younger age groups with an ACL injury and thus requires special consideration. Damage to the growth plates may lead to bone growth problems. For this group, ACL surgery can be delayed until the child is closer to reaching skeletal maturity.
-
Bleeding
Bleeding from acute injury to the popliteal artery.
-
Blood clot
Although rare, blood clot in the veins of the calf or thigh is a potentially life-threatening complications. A blood clot may break off in the bloodstream and travel to the lungs, causing pulmonary embolism or to the brain, causing a stroke.
-
Instability
Recurrent instability due to rupture or stretching of the reconstructed ligament or poor surgical technique is possible.
-
Stiffness
Knee stiffness or loss of motion has been reported by some patients after surgery.
-
Extensor mechanism failure
Rupture of the patellar tendon (patellar tendon autograft) or patella fracture (patellar tendon or quadriceps tendon autografts) may occur due to weakening at the site of graft harvest.
-
Kneecap pain
Postoperative anterior knee pain is especially common after patellar tendon autograft ACL reconstruction. The incidence of pain behind the kneecap varies greatly in studies, whereas the incidence of kneeling pain is often higher after patellar tendon autograft ACL reconstruction.
Rehabilitation After Anterior Cruciate Ligament (ACL) Injury
Physical therapy is a crucial part of successful ACL surgery, with exercises beginning immediately after the surgery. Much of the success of ACL reconstructive surgery depends on the patient’s dedication to rigorous physical therapy.
The goals for rehabilitation of ACL reconstruction include viz:
- Reducing knee swelling.
- Maintaining mobility of the kneecap to prevent anterior knee pain problems.
- Regaining full range of motion of the knee.
- Strengthening the quadriceps and hamstring muscles.
Conclusion
An ACL tear will only temporarily stop you from working your job or playing the sports you love. It is therefore not career-ending. Remember, your healing depends on your own choices: choices to use crutches, to have surgery or not, to work hard at your physical therapy